

演講題目
How Immigrants can be qualified for Medicare.(as early as 55)
新/老移民如何獲取紅藍卡資格?(最早是55)
4 Parts of Medicare A/B/C/D
– 紅藍卡的A/B/C/D四部分
Medicare AEO/IEP/OEP
– 紅藍卡的公開期/ 特殊公開期
———————–
– 新移民如何獲取紅藍卡資格?
如:需交10年稅
– 紅藍卡的A/B/C/D四部分
https://cainsguru.com/medicare-a-b-c-d/
– 紅藍卡的公開期/參加期
AEP/IEP/OEP(本次主要講述OEP 1/1-3/31)
如有時間會介紹(SEP 特殊公開期)
立即對比紅藍卡報價

1. 紅藍卡投保公開期 3月31日
https://www.medicare.gov/blog/medicare-advantage-open-enrollment-2020
2. 新冠疫情期間如何申請紅藍卡
3. 新移民如何申請紅藍卡?
例如:居住在國外的美國公民如何獲得紅藍卡的福利?
a. B部分 報銷項目
b. 哪個計劃覆蓋
https://www.medicare.gov/coverage/travel
EPIC (Humana 計劃詳情)
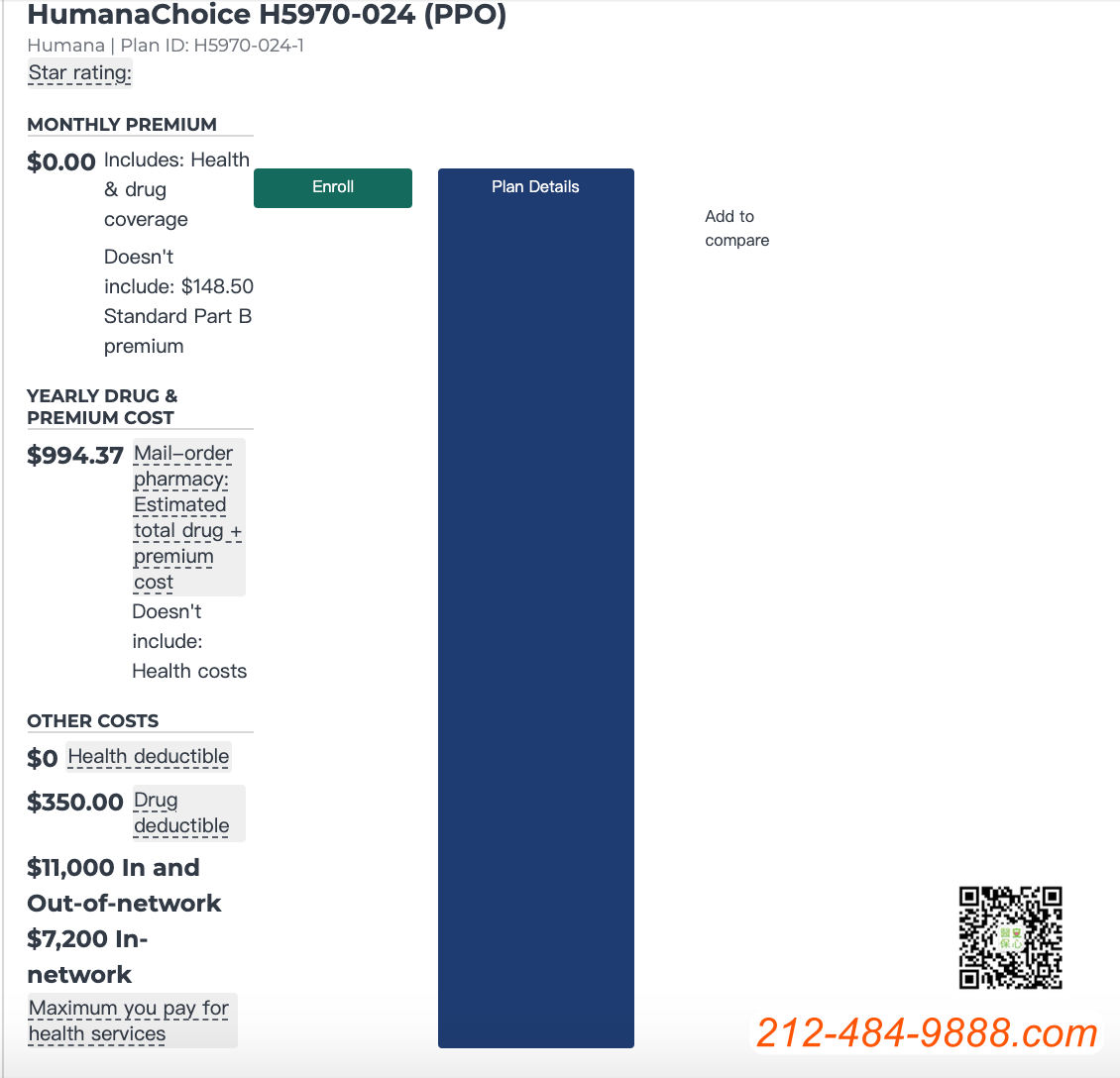
HumanaChoice H5970-024 (PPO)
Plan type: Medicare Advantage with drug coverage
Plan ID:H5970-024-1
Overview
PREMIUM
ESTIMATED YEARLY COSTS
MAXIMUM YOU PAY FOR HEALTH SERVICES
$7,200 In-network
Benefits & costs
DOCTOR SERVICESView Provider Network Directory
Out-of-network: $15 copay per visit
Out-of-network: $50 copay per visit
TESTS, LABS, & IMAGING
Out-of-network: $0-50 copay or 30% coinsurance
Out-of-network: $15-50 copay or 30% coinsurance
Out-of-network: $15-50 copay or 30% coinsurance
Out-of-network: $15-50 copay or 30% coinsurance
HOSPITAL SERVICES
$0 per day for days 6 through 90
$0 per day for days 91 and beyond
Out-of-network: $500 per day for days 1 through 7
$0 per day for days 8 through 90
Out-of-network: $50 copay or 30% coinsurance per visit
SKILLED NURSING FACILITY
$184 per day for days 21 through 100
Out-of-network: 30% per stay
Out-of-network: $0-50 copay or 30% coinsurance
AMBULANCE
Out-of-network: $290 copay
THERAPY SERVICES
Out-of-network: $50 copay or 30% coinsurance
Out-of-network: $50 copay or 30% coinsurance
MENTAL HEALTH SERVICES
Out-of-network: $50 copay
Out-of-network: $50 copay
Out-of-network: $50 copay
Out-of-network: $50 copay
OPIOID TREATMENT PROGRAM SERVICES
-
In-network:
- $40-$100 copay
-
Out-of-network:
- $50 copay
- 30% coinsurance
OTHER SERVICES
Out-of-network: 30% coinsurance per item
Out-of-network: 30% coinsurance per item
-
In-network:
- 20% coinsurance
-
Out-of-network:
- 20% coinsurance
Out-of-network: 30% coinsurance per item
Extra benefits & costs
HEARING
Out-of-network: $50 copay
Out-of-network: $0 copay
Out-of-network: $699-999 copay
Care to prevent or find problems with your teeth and gums.
Care to maintain or treat problems with your teeth and gums.
VISION
Out-of-network: $0 copay
Out-of-network: $0 copay
Out-of-network: $0 copay
MEDICALLY-APPROVED NON-OPIOID PAIN MANAGEMENT SERVICES
MORE BENEFITS
Optional packages
Deductible: N/A
Deductible: N/A
Drug coverage & costs
Plans group their drug lists into tiers. The table below shows your portion of the drug cost in certain tiers based on which coverage phase you’re in for this plan
| Tiers | Initial coverage phase | Gap coverage phase | Catastrophic coverage phase |
|---|---|---|---|
| Preferred Generic | $2.00 copay |
Generic drugs:25%Brand-name drugs:25%
|
Generic drugs:$3.70 copay or 5% (whichever costs more)Brand-name drugs:$9.20 copay or 5% (whichever costs more)
|
| Generic | $9.00 copay | ||
| Preferred Brand | $47.00 copay | ||
| Non-Preferred Drug | $100.00 copay | ||
| Specialty Tier | 26% |
Pharmacies
See the cost level to fill your drugs at the pharmacies you chose. You can also change pharmacies to see the cost level of other pharmacies in your area to find the lowest cost pharmacy.
| Mail Order Pharmacy | Costs vary based on the specific mail-order pharmacy | |
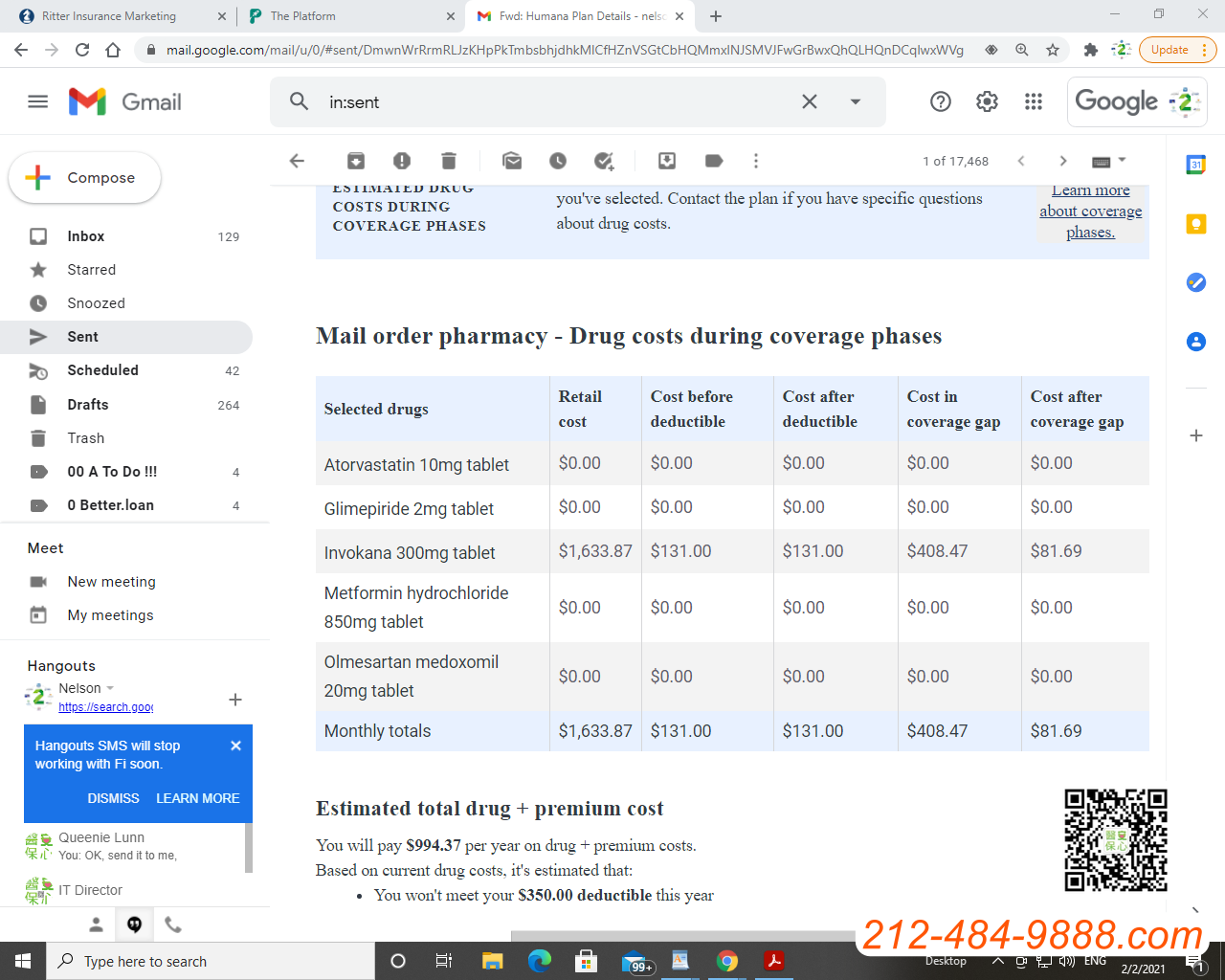
ESTIMATED DRUG COSTS DURING COVERAGE PHASES
The drug prices shown may vary based on the plan and pharmacy you’ve selected. Contact the plan if you have specific questions about drug costs.
Mail order pharmacy – Drug costs during coverage phases
| Selected drugs | Retail cost | Cost before deductible | Cost after deductible | Cost in coverage gap | Cost after coverage gap |
|---|---|---|---|---|---|
| Atorvastatin 10mg tablet | $0.00 | $0.00 | $0.00 | $0.00 | $0.00 |
| Glimepiride 2mg tablet | $0.00 | $0.00 | $0.00 | $0.00 | $0.00 |
| Invokana 300mg tablet | $1,633.87 | $131.00 | $131.00 | $408.47 | $81.69 |
| Metformin hydrochloride 850mg tablet | $0.00 | $0.00 | $0.00 | $0.00 | $0.00 |
| Olmesartan medoxomil 20mg tablet | $0.00 | $0.00 | $0.00 | $0.00 | $0.00 |
| Monthly totals | $1,633.87 | $131.00 | $131.00 | $408.47 | $81.69 |
You will pay $994.37 per year on drug + premium costs.
Based on current drug costs, it’s estimated that:
- You won’t meet your $350.00 deductible this year
Estimated monthly drug costs
This doesn’t include your monthly plan premium of $0.00.
| Time period | Estimated monthly drug costs |
|---|---|
| marzo | $131.00 |
| junio | $131.00 |
| septiembre | $323.90 |
| diciembre | $408.47 |
OTHER DRUG INFORMATION
| Selected drugs | Tier | Prior authorization | Quantity limits | Step therapy |
|---|---|---|---|---|
| Atorvastatin 10mg tablet | Tier 1 | |||
| Glimepiride 2mg tablet | Tier 1 | |||
| Invokana 300mg tablet | Tier 3 | |||
| Metformin hydrochloride 850mg tablet | Tier 1 | |||
| Olmesartan medoxomil 20mg tablet | Tier 2 |
藥物費用
Formulary
A list of prescription drugs covered by a prescription drug plan or another insurance plan offering prescription drug benefits. Also called a drug list.
HealthFirst Formulary Example
https://healthfirst.org/formularies
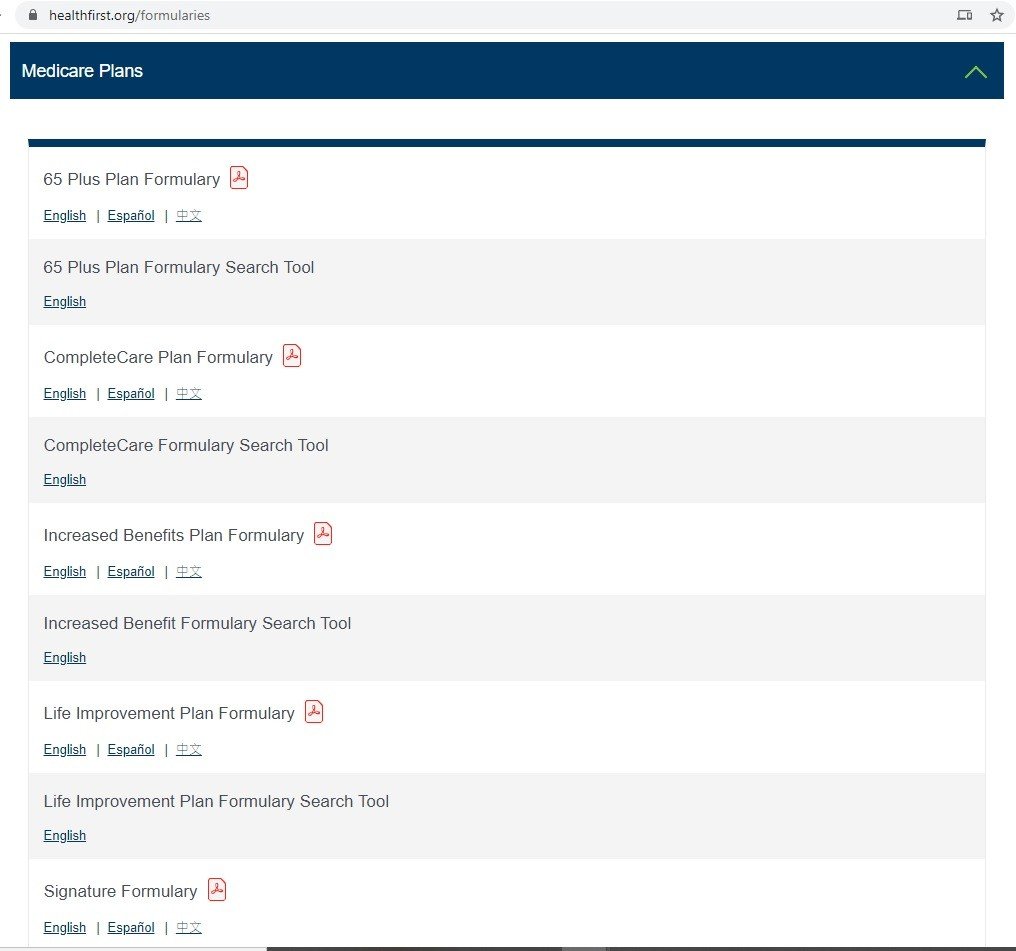
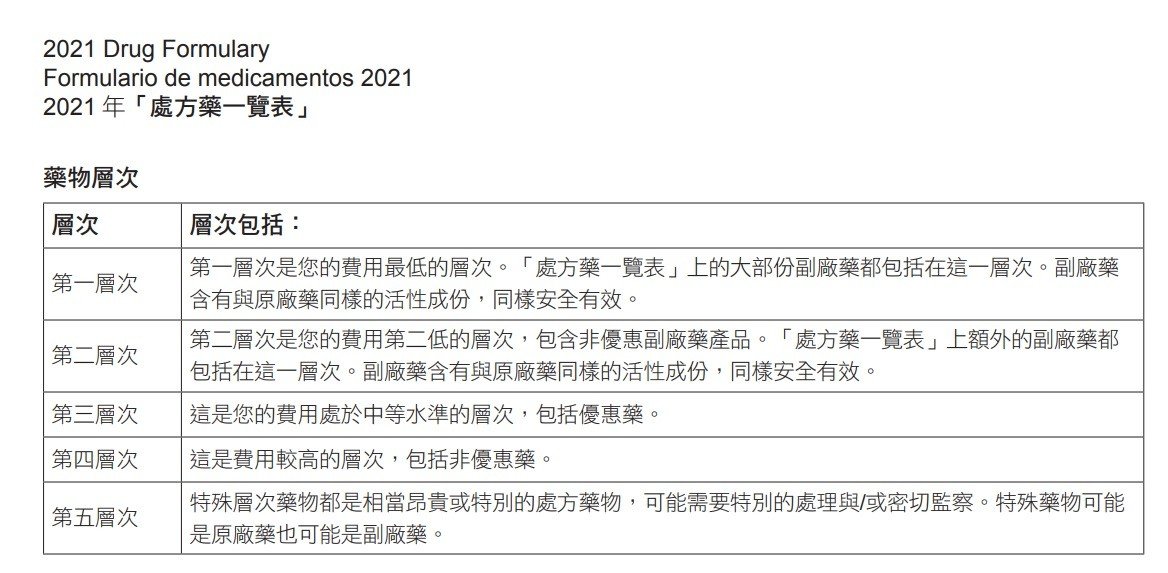
2021 Chinese Formularies List
https://assets.healthfirst.org/pdf_2d1357acc64ca13b1d3f0bda7f855a53?v=1006203326
什麼是共付額(Copayment)
共付額(Copayment) 是承保服務的固定金額,由患者在接受服務之前支付給服務提供者。可以在保險單中對其進行定義,並在每次獲得醫療服務時由被保險人支付。從技術上講,它是共同保險的一種形式,但在健康保險中有不同的定義,在健康保險中,共同保險是自付額達到一定限額後的百分比支付額。必須在保險公司支付任何保單利益之前支付。
根據藥物使用,成本和臨床有效性,將藥物劃分為四個,五個或六個類別之一,稱為共付額或共同保險等級。 我們的處方藥搜索可以根據您的福利計劃向您顯示適用於特定藥物的那一級別。
“四層配方”的共付額定義
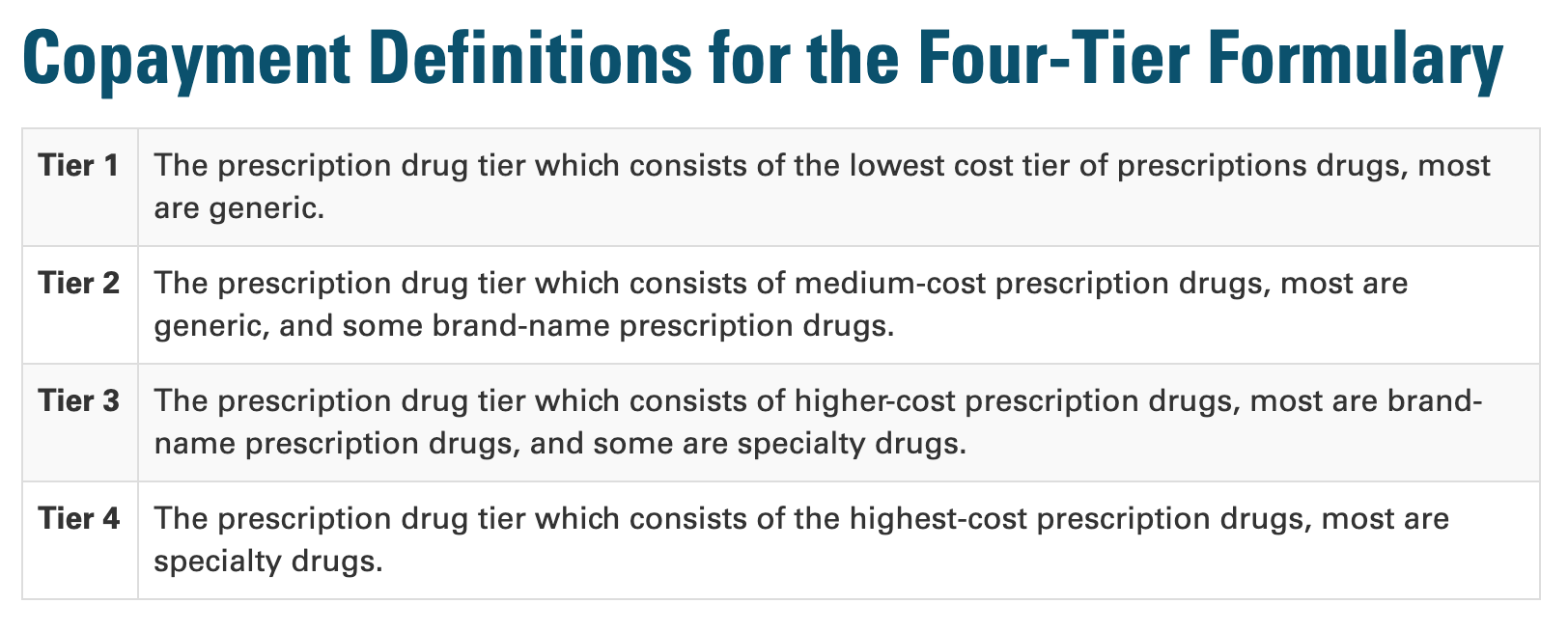
第1層處方藥:包括成本最低的處方藥,大多數是仿製藥
第2層處方藥:包括中等成本的處方藥,大多數是仿製藥,還有一些品牌原廠處方藥;
第3層處方藥:包括成本較高的處方藥,大多數是品牌原廠處方藥,還有些是特殊專業藥物;
第4層處方藥:包括成本最高的處方藥,大多數是特殊專業藥物。
Comparing Formulary Aetna vs HealthFirst
https://www.aetnamedicare.com/en/prescription-drugs/check-medicare-drug-list.html
Related posts:
 紐約[白卡/紅藍卡/紅藍白卡/聯邦醫療保險]申请💣3大陷阱須知💣解決方法?👍
紐約[白卡/紅藍卡/紅藍白卡/聯邦醫療保險]申请💣3大陷阱須知💣解決方法?👍 (55歲紅藍卡?新移民老人父母疫情版)
 紅藍卡的歷史
紅藍卡的歷史
 移民美國的父母-退休人士如何申請醫療保健(白卡/紅藍卡/紅藍白卡和F計劃)
移民美國的父母-退休人士如何申請醫療保健(白卡/紅藍卡/紅藍白卡和F計劃)
 美國聯邦醫療保險(紅藍卡)新移民/移民父母版
美國聯邦醫療保險(紅藍卡)新移民/移民父母版
 紅藍卡自費陷阱!哪些項目是紅藍卡不包的呢?
紅藍卡自費陷阱!哪些項目是紅藍卡不包的呢?
 紅藍卡優惠計劃各有不同 認清方案找到合適自己的計劃
紅藍卡優惠計劃各有不同 認清方案找到合適自己的計劃
 如何調整美國老人紅藍卡保險計劃
如何調整美國老人紅藍卡保險計劃
 (疫情版)配合家庭醫生 善用紅藍卡的省錢之道
(疫情版)配合家庭醫生 善用紅藍卡的省錢之道
 紅藍卡的承保內容、費用和重點是什麼?
紅藍卡的承保內容、費用和重點是什麼?
 申請紅藍卡有什麼注意事項?
申請紅藍卡有什麼注意事項?
 紅藍卡保費這麼高,值得買嗎?
紅藍卡保費這麼高,值得買嗎?
 川普/特朗普向紅藍卡老人發兩百元醫藥卡 惠及3300萬人!
川普/特朗普向紅藍卡老人發兩百元醫藥卡 惠及3300萬人!
 紅藍卡的A/B/C/D四大部分是什麼意思?有什麼作用呢?
紅藍卡的A/B/C/D四大部分是什麼意思?有什麼作用呢?
 【1張照片$500報酬】征求紅藍卡65歲以上模特兒照片
【1張照片$500報酬】征求紅藍卡65歲以上模特兒照片
 白卡2021重磅消息「老年人申請長期護理將大受影響」
白卡2021重磅消息「老年人申請長期護理將大受影響」
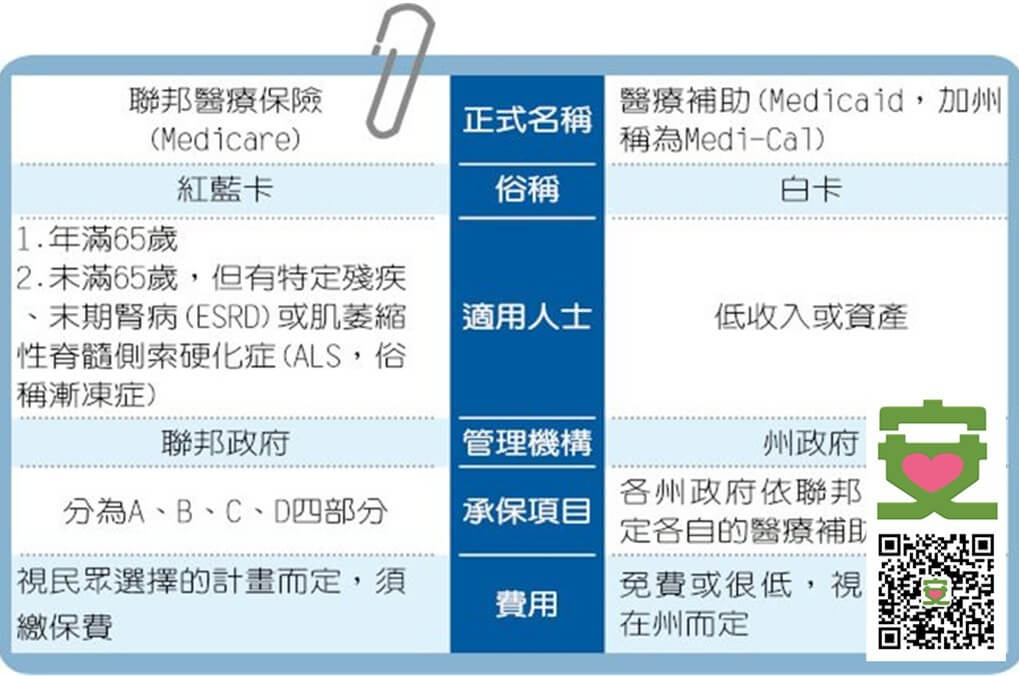 紅藍白卡 白卡和紅藍卡的區別是什麼
紅藍白卡 白卡和紅藍卡的區別是什麼
 究竟比爾蓋茨離婚跟你和我的👵🏻紅藍卡有什麼關係🤔
究竟比爾蓋茨離婚跟你和我的👵🏻紅藍卡有什麼關係🤔只需婚姻關係有10年或以上…